Lessons learned from the adaptations to the provision of contraception-related services to adolescents and young people during the COVID-19 pandemic: case studies from nine organisations in eight countries
Author
Dr Ahmed K. Ali
Dr Venkatraman Chandra-Mouli
Country
Democratic Republic of the Congo, Fiji, India, Myanmar, Namibia, Nigeria, Philippines, Uganda

Countries
Democratic Republic of Congo: Ailes du Coeur
India: MAMTA Health Institute for Mother and Child; Institute of Health Management, Pachod (IHMP)
Myanmar: Marie Stopes International
Uganda: Marie Stopes International
Namibia Planned Parenthood Association (NAPPA)
Fiji: Reproductive Family Health Association (RFHAF)
Philippines: Family Planning Association of the Philippines (FPOP)
Nigeria: Society for Family Health (SFH)
Key learning themes
• Organizations were able to nimbly adapt the provision of contraception services to overcome the obstacles created by the pandemic, using a wide range of methods, including digital and remote services, to reach the intended groups of adolescents and young people.
• Input received from young people, whether as beneficiaries or as contributors to programme design, proved essential in planning and implementing these interventions. In some cases, the adaptations went through many iterations to reach a point where they truly responded to the needs and preferences of adolescents and young people.
• Similar to the lessons learnt from the Provision of comprehensive sexuality education during COVID-19, there is a potential for these nimble adaptations to be used beyond the pandemic context, either by complementing or by substituting traditional programmes, especially in humanitarian contexts, but their effectiveness needs to be further evaluated
Background
Early in the COVID-19 pandemic, service disruptions and movement restrictions led to limited access to health, education and social services, including those related to adolescent sexual and reproductive health (ASRH). In many sites, health services were shut down and there were concerns that adolescents’ access to contraceptives may be seriously compromised during this period.
This brief provides a synthesis of lessons learnt from the nimble adaptations made by a number of organizations in order to maintain delivery of contraception-related services during the early stages of the COVID-19 pandemic, with a particular focus on adolescents and young people
Impact of COVID-19 onessential health services
Adolescents and young people in many places face barriers to obtaining the contraceptive services they need. To respond to this, the organizations mentioned in this brief make it easier for adolescents to obtain such services. Prior to the pandemic, they were able to access contraception services through the clinics operated by these organizations. When lockdowns and curfews were imposed in countries to curb the spread of COVID-19, the organizations found it very difficult to maintain the essential services they had previously been offering. However, many took practical measures, such as shifting to remote and digital services, while others adapted their service delivery modalities to continue providing in-person contraception services during the pandemic.
What was the intervention or activity?
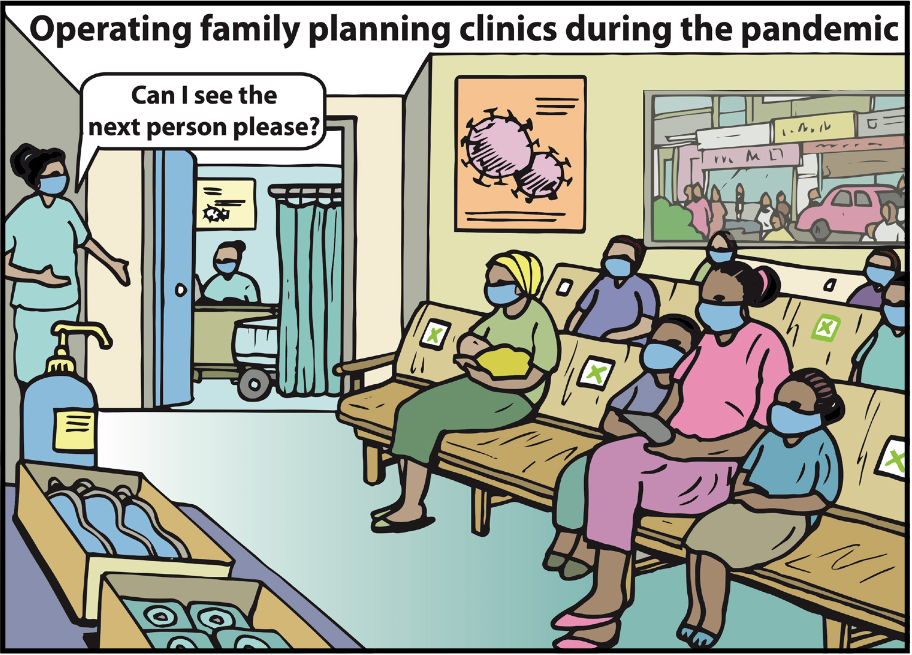
Most of the organizations that provided contraceptive services in their clinics did so in compliance with COVID-19 guidelines. The measures they used included using personal protective equipment, arranging appropriate seating to maintain physical distancing in waiting areas, reducing the number of clients per shift by including greater spacing between appointments, and adding shifts that were consistent with curfew timings and suitable for adolescent clients.
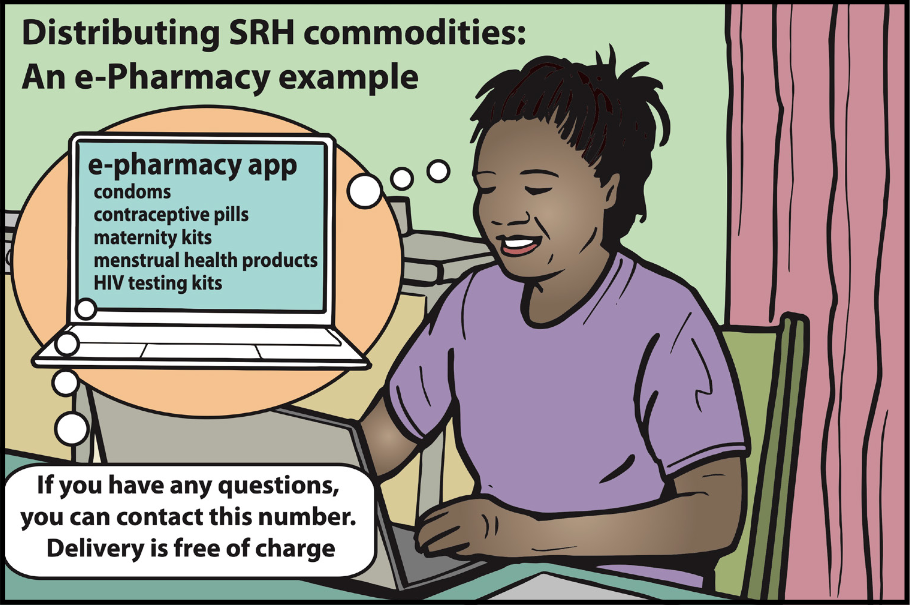
Other organizations provided alternative options for accessing contraceptives. For example, they installed condom dispensers as a quick “grab n’ go” at locations convenient to adolescents and young people. In addition, outreach workers or mobile clinics were employed to reach out and provide sexual and reproductive health services, including contraceptives, within nearby communities. Some organizations conducted household visits and provided contraceptives upon request. In addition to providing contraceptives, some of the organizations were able to provide counselling, either in person at their clinics, or remotely via online counselling.
Organizations made determined efforts to communicate the availability of these modified services to adolescents and young people using a variety of methods. They used messaging services, social media, helplines, outreach teams and youth volunteers to spread the information. Furthermore, they helped some organizations in scheduling services for appointments for referrals through messaging services or helplines as well.
Artwork prepared for and in conjunction with WHO. Artist: Graham Ogilvie, ogilviedesign.co.uk
How did this intervention / activity contribute to the maintenance of EHS?
Most organizations were able to circumvent the impact of shutdown on their services by adapting their service delivery mechanisms to comply with mandated COVID-19 measures within their settings. Others resorted to remote services in order to either complement existing services or to provide alternative options, including both remote and digital approaches, that could be accessed by adolescents.
What were the key challenges involved?
• Early in the pandemic, some cadres of health care providers, especially physicians and nurses, were shifted to serving as front-line health care providers for COVID-19 prevention and case management. This initially impacted the availability of services. Organizations had to adapt their scheduling or resort to providing partial services to address this staff shortage.
• Furthermore, early in the pandemic, there was an assumption among the general public that health services would be closed indefinitely. This may have deterred adolescents and young people from accessing the adapted services when they were made available. Once services were resumed, different communication methods were used to inform them about the availability of services and changes in service delivery modes.
• In many sites, adolescents and young people faced movement restrictions. To respond to this, organizations provided remote or digital services to enable their access to contraception-related services.
Artwork prepared for and in conjunction with WHO. Artist: Graham Ogilvie, ogilviedesign.co.uk
Disclaimer
These HLH action briefs and learning briefs are presented for learning purposes only. Their content has been developed by the organization and author(s) named and as such does not necessarily represent the policies or approaches of WHO.